
Patient: XXXXXXXX XXXXXXX
Subjective Complaints:
38 Year Old Male who presents with Lumbar (L3-L5) Pain which symptoms are described as a sharp localized pain in the low back with periodic buttox pain. There are general fatigue symproms in the body which occur on a daily basis. The more he walks, and stands, the greater the discomfort.
Past Medical History: Unremarkable
Past Surgical History: None except for oral dental surgery
Occupational History: Works in a inventory supply warehouse 8 hours a day. Symptoms seem to intensify around 3 PM and last through the evening.
Objective Findings:
Examination is performed by evaluating the plane of the deformities.
Examination is performed by evaluating the plane of the deformities.
Weight 230 pounds BP 135/85 Pulse 82
Orthopedic Examination
Stance Examination:
Frontal Plane
- Knee position medially deviated (moderate) Coxa Vara Genu Valgum)
- There is a Left Pelvic Drop on palpation suggesting a possible leg shortage
- There is palpable pain in the lower lumbar quadrant which seems more intense ion the right side.
- Both feet are fully pronated
Lateral Plane
- The knees appear hyperextended (Genu Recuvatum) bilaterally
- The lumbar spine is in lordosis
- There is moderate abdominal distension with possible abdominal hernia and no protrusion or palpable viscera.
Transverse Plane
- There is a 12 degree abducted midline position equally
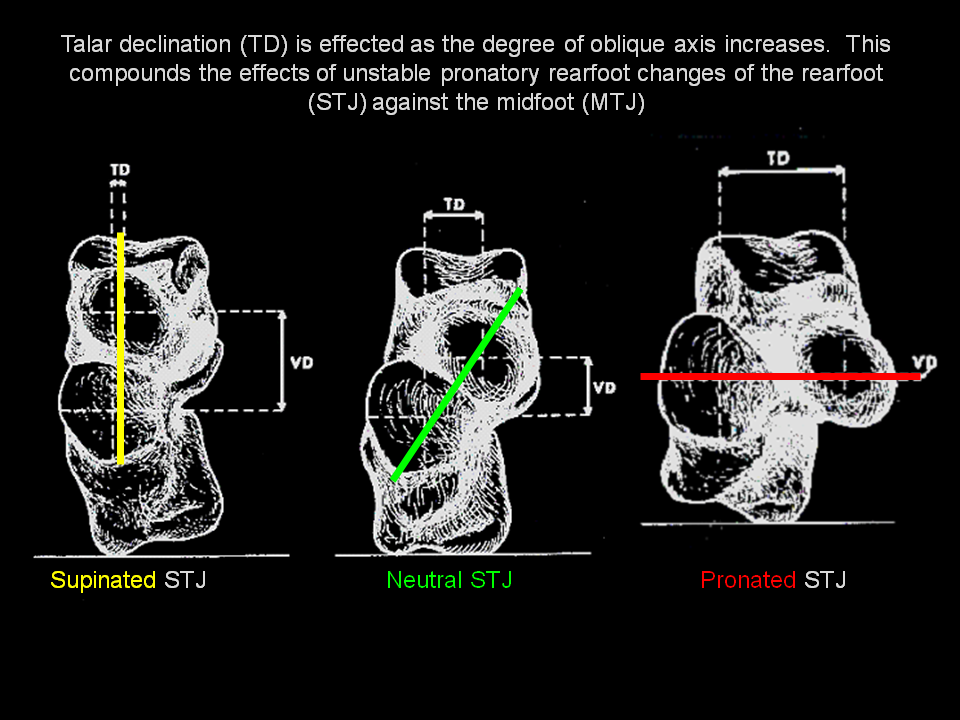
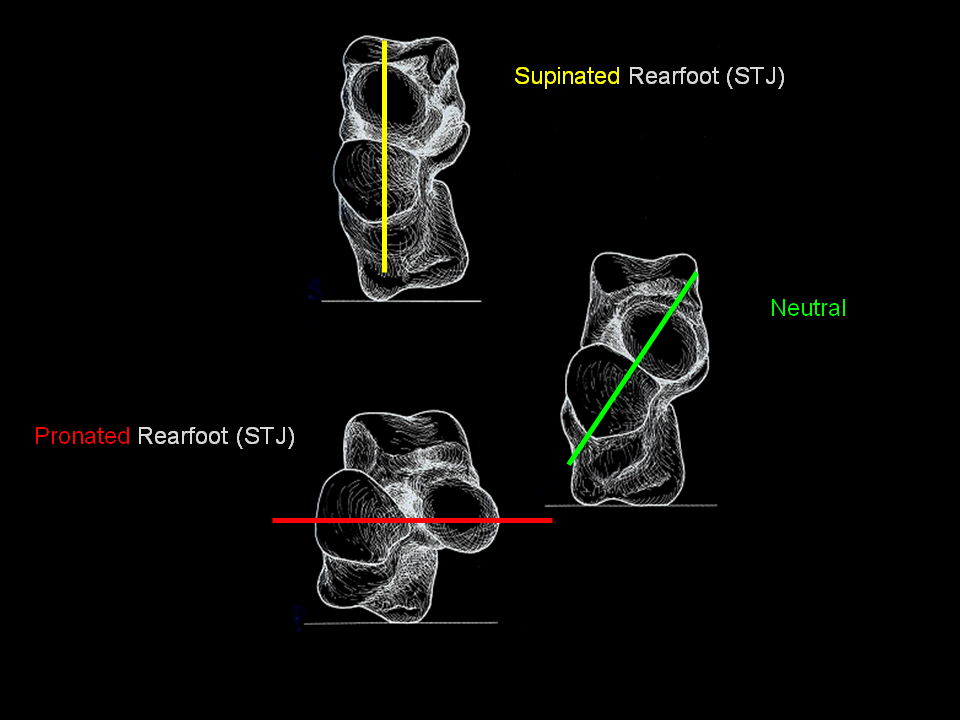
- The rearfoot is everted bilaterally
Dynamic Examination:
- There appears to be a right shoulder drop
- The patients gait is pronated
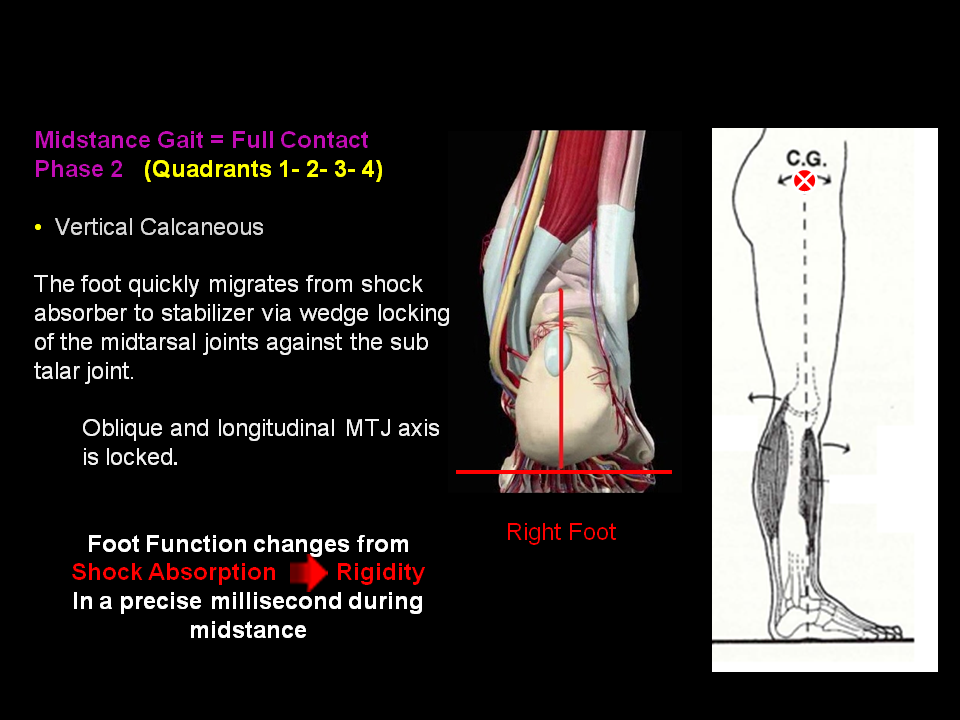
- There is extensive transverse internal limb rotation from heel contact through midstance
Structural Examination:
- Patient has moderate Hallux Abductus with 1st Ray hypermobility
- The 5th Ray is also hypermobile bilaterally
- There is moderate Tibial Varum bilateral
- Range of motion of knee and hips are symmetrical with no crepitation
Range of Motion:
- Hypermobility of foot joints
- Same for soft tissues
Gait Examination:
- Suggest excessive pronatory pathomechanics of both feet
- Patient has an antalgic Gait favoring the left leg
3D Weight Bearing Kinematic Examination using 3DO Imaging:
- Static Analysis reveals weight shifting to the right limb suggesting left leg shortage. The weight distribution of the left leg is 40% and 60% for the right leg. There is high impact loading in the plantar calcaneal areas R>L. There is also high impact loading on plantar 2,3,4 MPJ bilateral. 1st and 5th MPJ areas fail to load proper percentage of weight.
- Dynamic Analysis reveals heel contact everted on right more than left. Mass migration fails to load on the 1st ray and instead migrates through the lesser metatarsals. The 1st and 5th rays are hypermobile bilaterally.
Assessment - Diagnosis: Key is to list Diagnosis based on Treatment for best payment. Send in Outcome Measurement Report with billing for objective justification.
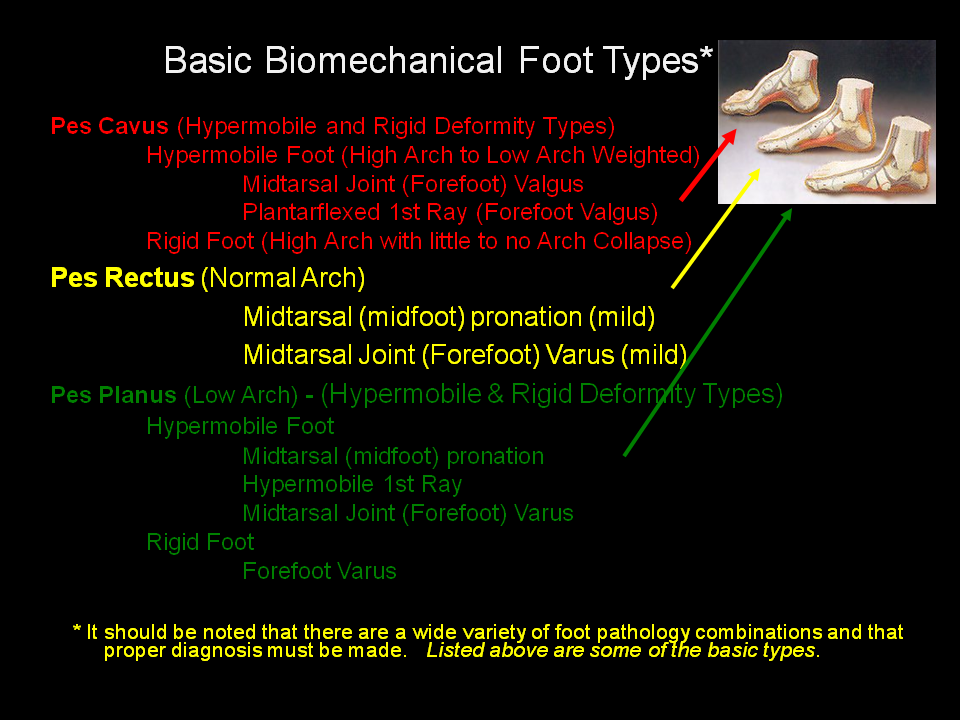
- Pes Planus Bilateral
- Metatarsalgia with Metatarsal Depression 2,3,4 bilateral
- Antalgic Gait
- 7 degress Midtarsal Joint Varus Left and 9 degrees Right
- Hypermobile 1st Ray bilateral
- Tibial Varum
- Hamstring Equinus
- Coxa Vara Genu Valgum
- Unilateral Short Leg Syndrome Left
- Lumbar Disc Syndrome L 4-5
- Lumbar Lordosis
Treatment Plan:
- 3D Weight Bearing Kinematic Analysis
- Gait Analysis
- Video Analysis
- Casting
Prognosis:
- Excellent - Treatment of biomechanical etilogy will provide a restabilization of pathomechanical diseases in this patient and prevent surgery of the spine.
- See Outcome Measurement report (attached)
Followup:
- Recommend 6 month followup analysis to evaluate progress and provide adjuetment to current biomechanical program.
Discussion:
Hypermobile Pes Planus feet with associated midtarsal joint varus pose a significant load bearing problem for upper extremity joints as this foot creates a significant amount of internal leg rotation as a result of pronatory movement of the feet. Treating and stabilizing the biomechanical motion is critical as well as elevating the short leg. Failure to treat the mechanical disease leaves the patient vunerable to surgery and toxic oral anti-inflammatory treatments which will not treat the cause of disease.















{kind=link}