
Hypermobile versus Rigid Pathomechanics
Hypermobile versus Rigid deformities are functionally opposed relative to the dynamics of biomechanical and ergonomic disease. In general, Hypermobile feet have too much motion and Rigid feet have restricted motion.
The foot has two fundamental functions;
- Act as a shock absorber along with the knees as the body impacts the floor
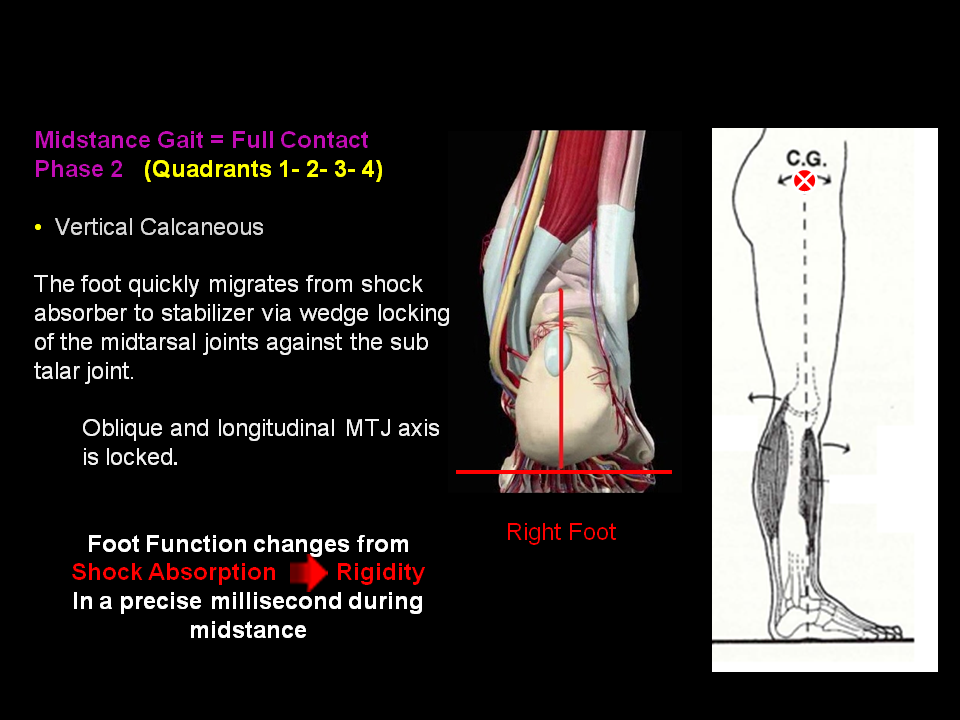
- When Midstance begins (forefoot contact), the foot changes in a millisecond into a Stabilizer through effective Wedge Joint Locking of the Rearfoot, (Sub Talar Joint) against the Midfoot, (Midtarsal Joints and 1st Ray (Navicular, Medial Cuniform, 1st Metatarsal, and Hallux). This is assisted from reactive ground force through the plantar foot, Failure of proper locking, leaves the foot unstable and there is resultant excessive limb rotation (Midstance through Propulsion).
The Custom Bio-Engineered Devices must be able to adequately position rearfoot loading which maximizes Sub Talar Joint function and wedge locking of the midtarsal joints in a precise millisecond of time while enable the 1st Ray to properly load during midstance. At the same time, allow the digits and hallux to grasp and propel weight.
The most common type seen in clinical practice is the hypermobile foot and limb syndrome.
The most common type seen in clinical practice is the hypermobile foot and limb syndrome.
This condition presents itself with a foot with excessive motion and a limb with excessive motion at articular joint surfaces. The patient presents with excessive mobility of joints of the feet and relative transfer of abnormal pronatory range of motion in the form of excessive internal leg rotation from he'll contact into mid stance.
These patients will present with a unstable he'll contact with rapid midtarsal joint subluxation and pronation secondary to lack of midtarsal joint locking in addition to hypermobility of the first ray.
These patients will also demonstrate apropulsive toe off due to lack of plantarflexion of the first ray from mid stance into propulsion due to hypermobility of joints as well as lack of extrinsic pull of the peroneus longus and assistance of the posterior tibial tendons.
In general, hypermobile feet translate into excessive internal limb rotation creating excessive pathomechanical disease in the knees, hip, and spine due to excessive pelvic rotation. When the normal axis of motion is disturbed, then the joint(s) must work off their normal axis and then injury and disease sets in over time (Wolf's Law).
Objective assessment only goes so far, and it is necessary to get finite close kinetic chain evaluation through the intervention of 3-D weight-bearing kinematic imaging which evaluates (7) area of important areas of load bearing mechanics;- Mass Displacement Analysis
- Body Balance in all 3 planes
- Pressure Load (Linear and Sheer Pressure)
- Motion Analysis (Velocity)
- Symmetry
- Gait Analysis
- 3D Plantar Foot Geometry
How we see Biomechanical Anatomy (Transverse Plane)
4 Anatomical Quadrants with different and unique functions

Center Point of Balance in all three body planes

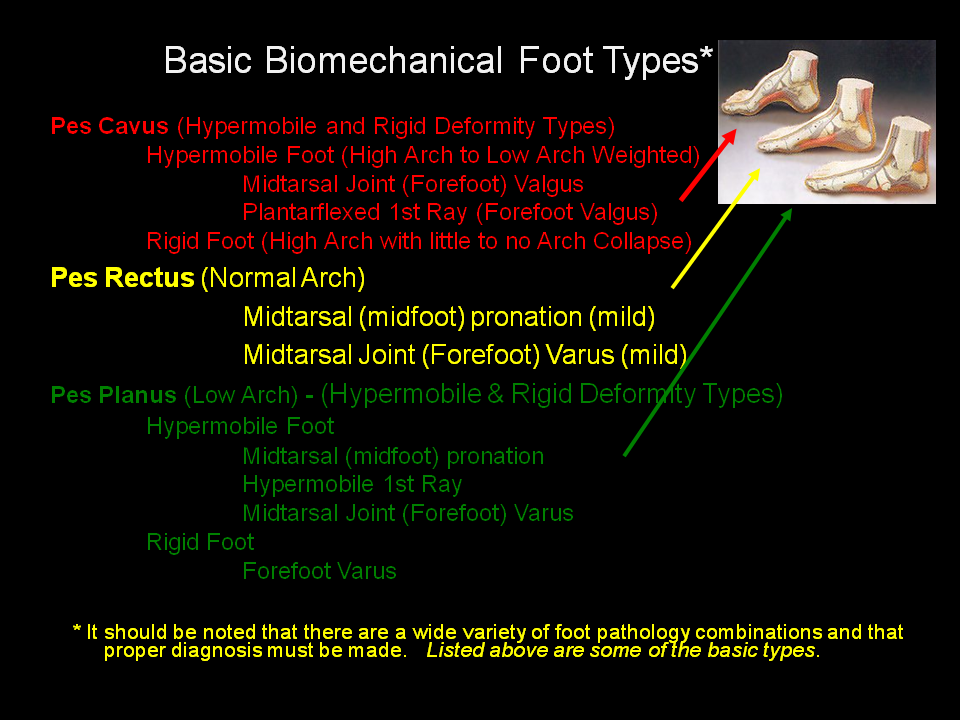
Foot Types
Midtarsal Joint Varus versus Valgus Pathomechanics (Frontal Plane)
Midtarsal Joint Varus is the most common biomechanical disorder.

Midtarsal Joint Varus
Non Weight Bearing = Forefoot Inverted - Weight Bearing = Everted Rearfoot
This deformity can be present in a Pes Planus (flatfoot) or a Hypermobile Pes Cavus (high arch off weight bearing and low arch on weight bearing).

Transverse Plane - Midtarsal Joint Axis
(Oblique and Longitudinal)


Lateral Plane Midtarsal Joint Axis
(Oblique and Longitudinal)

Hypermobile 1st Ray (Navicular - Medial Cuniform - 1st Metatarsal - Hallux)
Non Weight Bearing = Forefoot Normal - Weight Bearing = Everted Rearfoot
The difference is that in weight bearing, the 1st Ray's is excessively hypermobile and fails to plantarflex during midstance leaving the lesser metatarsals vunerable to increased impact loading.

{kind=link}


Both the Midtarsal Joint Varus and Hypermobile 1st Ray deformities create unstable and excessive transverse plane limb rotation leading to knee, hip and spinal pain. Control is critical and requires Dynamic 3D assessment.
____________________________________________
Midtarsal Joint Valgus
Non-Weight Bearing = Forefoot Everted - Weight Bearing = Inverted Rearfoot
Commonly seen with Cavus and Rigid Plantarflexed 1st Ray deformities

Subtalar Pathomechanics
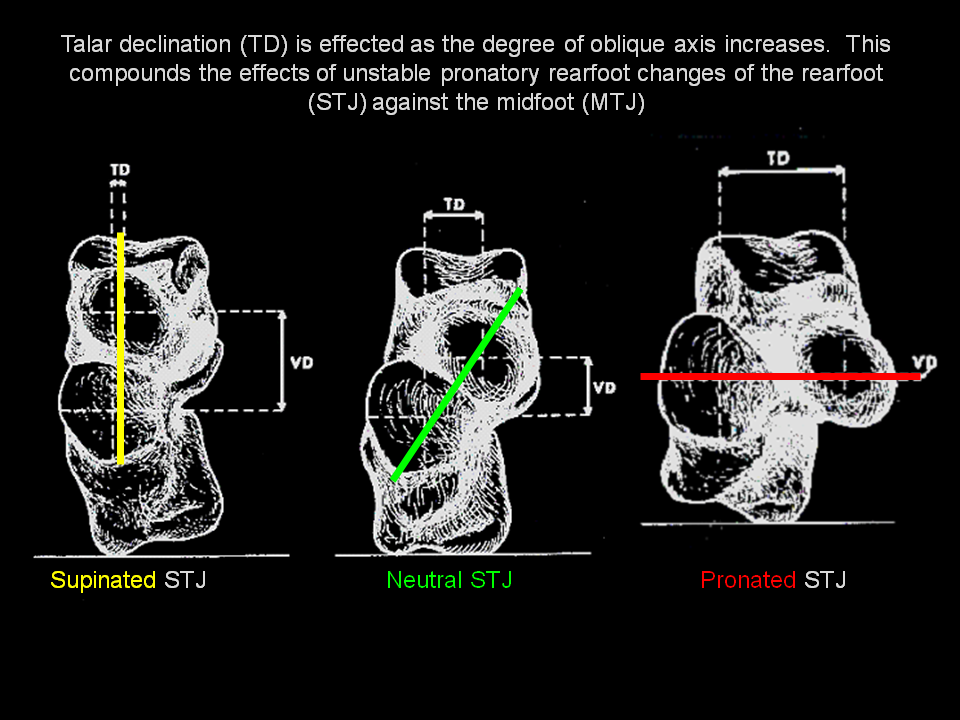
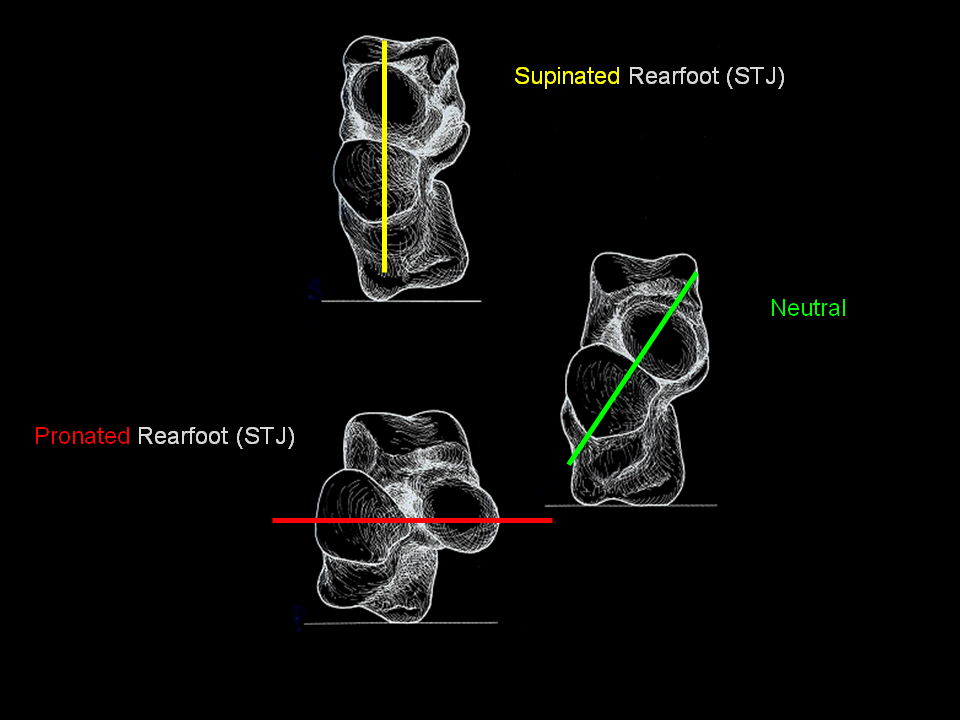
The articulation between the Talus and Calcaneous makes up the Sub Talar Joint. It is a trimotion joint and is responsible for wedge joint locking of the Midtarsal Joints during midstance. It's function is affected by many factors including Lateral Plane Equinus influences.
The more the oblique the articulation, the more unstable and pronated influences will effect the rearfoot and midfoot.
STJ Range of Motion - (example)

Lateral Plane Influences (Equinus)

General Commments on Body Plane Pathomechanics
- Think 3D - Everything occurs in all three body planes
- Understand the influences of extrinsic and intrinsic musculoskeletal influences
Equinus and its effect on Pathomechanics
- Equinus usually involves the Gastrocnemius - Soleus - Hamstrings
- Equinus is a major deforming force on the body, (Spine - Pelvis - Hip - Knee - Foot). It accelerates the velocity of pronation resulting from hypermobility due to the forward displacement of mass.
- It causes prematire forefoot loading and unlocking of the Subtalar and Midtarsal Joints not to mention the 1st Ray. .
- It affects spinal, knee and hip function dramatically.
- It is a major component to Spinal Disease and pain
- It is a component to acceleration of knee instability and disease

Structural (Bone/Osseous) Disease and its effects on Body Pathomechanics
- Leg Shortages (Pelvis fromntal Plane)
- Tibial Torsion (Transverse Plane)
- Tibial Varum (Frontal Plane)
- Acetabular to Femoral Shaft Deviations - Coxa Vara / Coxa Valgum - (Frontal Plane)
- Calcaneal Varum (Frontal Plane)
- 1st Ray (Metatarsus Primus Varus) - Transverse Plane
- 1st MPJ Articular Adaption (Vallux Abducto Valgus) Transverse and Frontal Plane
- Hammertoes
- Calcaneal Exostosis (Heel Spur) - Lateral Plane
No comments:
Post a Comment